This week the Australian Royal Commission into Antisemitism and Social Cohesion is a mixed bag, but it’s all very close to home. The Royal Commission is talking about learning and educational resources today, for example, so I have to watch. I need to know how what I do (or did when I had lots of teaching and do on the rare instance I’m back teaching) fits into good practice. I also need to be critical of what everyone else is doing. Not bad-critical, but aware-critical. Today then, is an in-service for education outside the tertiary sector.
Then there are three days of things I know but need to understand better. Learning and education require this, and just because I’ve been excluded from much of the education I used to give, doesn’t absolve me from learning and updating. It’s ironic that I’m updating my understanding of why I’ve been excluded, but that’s only a small slice of a vast pie about education in Australia and how it fits with being Jewish in Australian.
Friday, as I told everyone on Facebook, is my personal hellscape, because it’s about antisemitism in the Arts and Creative sector. It’s not my once-life and hope-to-be life: it’s my current everyday. I say “hope-to-be” but the silencing and how Jewish creatives now live in a different world to most others hasn’t yet been tackled and may not be tackled. The focus here is on the hate, not the side effects of hate. The introduction for this week (by counsel assisting) has already noted how many of us are isolated and drifting thanks to the antisemitism, which is a big advance.
Outside the Royal Commission, people are blaming Jews for all kinds of things still. The new thing they (those who hate) have is an assessment of the Royal Commission while not paying any attention to what everyone says in it. The investigation into antisemitism itself becomes an excuse for antisemitism. I read something that suggests that people who do this enjoy hating. I wish they were wrong.
I asked my Facebook followers to consider. “Anyone who has political opinions on these subjects, listen to the evidence at the RC first and maybe think on how things affect me and other Australian Jews in your vicinity. Is your opinion on my page more important than my safety or emotional stability? Your choice, of course, but I’d rather you made it an educated choice.”
None of this was going to be today’s post. I had completely different ideas. But in the background, I’m hearing a rabbi talking about healing the staff at Bankstown Hospital, which is known to be antisemitic. So many people are taking their religion off their hospital record, for their own safety. There was discussion in Sydney about even finding alternates to hospitals because of safety. The State government is now talking about what to do. Healing is going to take a long time. Safety is still an issue. At least, however, more people are now talking about this.
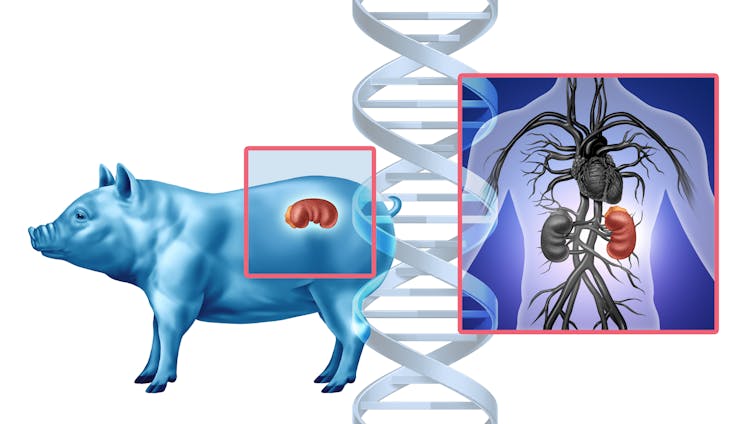
In a New York operating room one day in October 2025, doctors made medical history by transplanting a genetically modified pig kidney into a living patient as part of a clinical trial. The kidney had been engineered to mimic human tissue and was grown in a pig, as an alternative to waiting around for a human organ donor who might never come. For decades, this idea lived at the edge of science fiction. Now it’s on the table, literally.
A decade ago, scientists were chasing a different solution. Instead of editing the genes of pigs to make their organs human-friendly, they tried to grow human organs – made entirely of human cells – inside pigs. But in 2015 the National Institutes of Health paused funding for that work to consider its ethical risks. The pause remains today.
As a bioethicist and philosopher who has spent years studying the ethics of using organs grown in animals – including serving on an NIH-funded national working group examining oversight for research on human-animal chimeras – I was perplexed by the decision. The ban assumed the danger was making pigs too human. Yet regulators now seem comfortable making humans a little more pig.
Why is it considered ethical to put pig organs in humans but not to grow human organs in pigs?
Urgent need drives xenotransplantation
It’s easy to overlook the desperation driving these experiments. More than 100,000 Americans are waiting for organ transplants. Demand overwhelms supply, and thousands die each year before one becomes available.
For decades, scientists have looked across species for help – from baboon hearts in the 1960s to genetically altered pigs today. The challenge has always been the immune system. The body treats cells it does not recognize as part of itself as invaders. As a result, it destroys them.
A recent case underscores this fragility. A man in New Hampshire received a gene-edited pig kidney in January 2025. Nine months later, it had to be removed because its function was declining. While this partial success gave scientists hope, it was also a reminder that rejection remains a central problem for transplanting organs across species, also known as xenotransplantation.
Decades of research have led to the first clinical trial of pig kidney transplants.
Researchers are attempting to work around transplant rejection by creating an organ the human body might tolerate, inserting a few human genes and deleting some pig ones. Still, recipients of these gene-edited pig organs need powerful drugs to suppress the immune system both during and long after the transplant procedure, and even this may not prevent rejection. Even human-to-human transplants require lifelong immunosuppressants.
That’s why another approach – growing organs from a patient’s own cells – looked promising. This involved disabling the genes that let pig embryos form a kidney and injecting human stem cells into the embryo to fill the gap where a kidney would be. As a result, the pig embryo would grow a kidney genetically matched to a future patient, theoretically eliminating the risk of rejection.
Cross-species organ growth was not a fantasy – it was a working proof of concept.
Ethics of creating organs in other species
The worries motivating the NIH ban in 2015 on inserting human stem cells into animal embryos did not come from concerns about scientific failure but rather from moral confusion.
Policymakers feared that human cells might spread through the animal’s body – even into its brain – and in so doing blur the line between human and animal. The NIH warned of possible “alterations of the animal’s cognitive state.” The Animal Legal Defense Fund, an animal advocacy organization, argued that if such chimeras gained humanlike awareness, they should be treated as human research subjects.
The worry centers on the possibility that an animal’s moral status – that is, the degree to which an entity’s interests matter morally and the level of protection it is owed – might change. Higher moral status requires better treatment because it comes with vulnerability to greater forms of harm.
Think of the harm caused by poking an animal that’s sentient compared to the harm caused by poking an animal that’s self-conscious. A sentient animal – that is, one capable of experiencing sensations such as pain or pleasure – would sense the pain and try to avoid it. In contrast, an animal that’s self-conscious – that is, one capable of reflecting on having those experiences – would not only sense the pain but grasp that it is itself the subject of that pain. The latter kind of harm is deeper, involving not just sensation but awareness.
Thus, the NIH’s concern is that if human cells migrate into an animal’s brain, they might introduce new forms of experience and suffering, thereby elevating its moral status.
How human do pigs need to be for them to be considered part of the human species? AP Photo/Shelby Lum
The flawed logic of the NIH ban
However, the reasoning behind the NIH’s ban is faulty. If certain cognitive capacities, such as self-consciousness, conferred higher moral status, then it follows that regulators would be equally concerned about inserting dolphin or primate cells into pigs as they are about inserting human cells. They are not.
In practice, the moral circle of beings whose interests matter is drawn not around self-consciousness but around species membership. Regulators protect all humans from harmful research because they are human, not because of their specific cognitive capacities such as the ability to feel pain, use language or engage in abstract reasoning. In fact, many people lack such capacities. Moral concern flows from that relationship, not from having a particular form of awareness. No research goal can justify violating the most basic interests of human beings.
If a pig embryo infused with human cells truly became something close enough to count as a member of the human species, then current research regulations would dictate it’s owed human-level regard. But the mere presence of human cells doesn’t make pigs humans.
The pigs engineered for kidney transplants already carry human genes, but they aren’t called half-human beings. When a person donates a kidney, the recipient doesn’t become part of the donor’s family. Yet current research policies treat a pig with a human kidney as if it might.
There may be good reasons to object to using animals as living organ factories, including welfare concerns. But the rationale behind the NIH ban that human cells could make pigs too human rests on a misunderstanding of what gives beings – and human beings in particular – moral standing.
This article was updated to correct the location and date of the first pig kidney transplant clinical trial.
I just posted about one of my novels, Borderlanders, on Facebook. Let me share that post, and let me add to it.
Memories…
This was the book wanted by readers on FB. I noted (on FB, obviously) that my academic stuff had given me a way of writing a novel with a chronically ill protagonist where the protagonist remains the hero, is not cured, is not killed, and is not replaced. I was going to teach this method to others, but first COVID intervened and then antisemitism. I don’t get to teach much, these days. I may have to write another novel, having said this, because I learned so much in writing the novel that I could now write a much better one.
What’s very strange is, during these 5 years, more people I know have the illness my character had, due to long COVID. I’ve had it since I was in my twenties, but I’m one of the fortunate ones for whom it goes into abeyance. Right now, I’m trying to coax it back to sleep. Not everyone has that luxury, which is another reason why I should write another novel. Not yet, though. While it’s awake, every moment of every day is not straightforward, and I am behind on all my fiction.
This mysterious illness was known as chronic fatigue in Australia in the late 1980s, but these days it’s called ME and the fatigue is just a symptom. We know a lot more about it. One thing we know is why walking up the street can be so impossible. For some of us it can set the illness back, and for others it can destroy life entirely. This is why I consider myself so fortunate. I may have to not do much for a few months, but after that time I can do a little more and then a little more. This is just as well, because it’s only one of several illnesses I have and I have this daft desire not to be bedridden or die young.
For me, the most annoying symptom is when my executive function is not working. I lose time (sometimes weeks) and can’t do simple things. Oddly, I can still write books.
I always tell folks, do not assume someone can or cannot do a thing when they are ill. Ask them. And ask them each and every day if you must, because the small everyday can change. Some days I can walk up the street and back and I can write 6,000 words. Other days I can hardly get out of bed.
The illness is not just part of our everyday, it becomes part of who we are, for better or for worse.
I would like to see a superhero who has ME. It would be such a wonderful thing, watching them change the world… on days they can do more than toddle. And seeing how other people respond to the wild level of change they see when a powerful person has to watch what they do every minute would provide a great sub-text to a movie. It’s quite a different set of options than those for someone who cannot walk without assistance, or someone completely confined to bed who uses their amazing telepathic abilities to run the world.
There are so many amazing stories in the lives of the people we mostly prefer not to see. I now want to see a whole sequence of superhero movies or a TV series that focuses on those lives. There is a different sort of heroicism when one is not visible and has to fight just to get through the everyday, especially when they do astonishing things. Most of those astonishing things are attributed to someone else, because, of course, the invisible and half-seen can’t possibly be the heroes we dream of. Except, of course, they are. I get through my illnesses because of those people. Some of them are role models and some of them help when others don’t even begin to see that I might not be able to ask for help when things are bad.
One thing about this non-extent show: costumes would be far too problematic for some of the hidden heroes. So would heroic stances and being randomly interviewed by reporters. It would be such a different and fascinating set of stories.
In real life, I’ve met these invisible people in essential services. From a desk or from home they make a lot of the everyday possible for so many other folk.
Yet, the U.S. is different in a meaningful way. Here, abortion has historically been framed as a personal right to privacy. In many other countries I’ve studied, abortion is viewed more as a collective right that is inextricably tied to broader social and economic issues.
Initially, for some of those autocratic leaders, limiting access to abortion and contraception was a strategy to gain the approval of the nation’s religious leaders. The Catholic Church held great power in Italy and Spain, as did the Orthodox Church in Romania. At the time, these faiths opposed artificial birth control and still believe life begins at conception.
Restrictions on reproductive rights also aimed to increasebirth rates following two world wars that had stamped out some of the population, particularly in the Soviet Union and Italy. Many political leaders saw procreation as a national duty. They designated women – white, heterosexual women, that is – specific roles, primarily as mothers, to produce babies as well as future soldiers and workers for their regimes.
In the past two decades, countries in Europe and the Americas have been following this recognizable pattern. Nicaragua and Poland have both banned abortion. Hungary, Turkey and Russia have all clamped down on access to it.
Restricting reproductive freedoms has helped Hungary’s Viktor Orbán, Russia’s Vladimir Putin and Turkey’s Recep Tayyip Erdoğan stoke lasting political divisions within society that help them consolidate their own power.
These politicians have also taken power away from a significant portion of the population by reinstating earlier, fascist-era restrictions on bodily autonomy. As feminist scholars have pointed out, strong reproductive rights are central to functioning democracies.
Restrictions on reproductive freedoms often necessitate other kinds of restrictions to enforce and maintain them. These might include free speech limits that prohibit providers from discussing people’s reproductive options. Criminalizing political dissent enables the arrest of people who protest restrictions on reproductive freedoms. Travel bans threaten prison time for individuals who help young people get abortion care out of state.
When these civil liberties weaken, it becomes harder to defend other rights. Without the right to speak, dissent or move freely, people cannot engage in conversations, organize or voice collective grievances.
Putting the US in a global context
In 2022, the U.S. joined the likes of Poland and Hungary when the Supreme Court overturned Roe v. Wade, ending 50 years of federal abortion protections.
President Donald Trump was not in power when this happened. Yet the Supreme Court’s conservative majority was shaped during his first term.
Since then, both the second Trump administration and many states have enacted their own regulations or bans on abortion. This has created a divided country where in some states abortion is as restricted as it is under some of the world’s most autocratic regimes.
Yet, there’s a key difference.
In the U.S., abortion is viewed by the law and the public as a matter of individual rights. The debate often boils down to whether a person should be allowed to terminate their pregnancy.
In many other contexts, reproductive rights are understood as a collective good that benefits all society – or, conversely, harms all society when revoked.
This perspective can be a powerful driver of change. It’s how, for example, women’s and feminist groups in places such as Argentina, Colombia and Mexico have successfully pressured their governments to decriminalize abortion in recent years.
The Latin American feminist activists have also documented how restricting abortion intensifies authoritarianism and worsens both individual and collective rights.
In a region where many citizens remember life under military dictatorship, highlighting the relationship between abortion and authoritarianism may be particularly galvanizing.
This was basically what the mainstream pro-choice movement advocated for at the time. White feminists saw abortion rights as a personal liberty. This framing has real limitations.
As Black and brown reproductive justice advocates have long pointed out, Roe never served women of color or poor people particularly well because of underlying unequal access to health care. Their work has, for decades, illustrated the strong connection between racial, economic and reproductive justice, yet abortion is still largely regarded as solely an individual issue.
When debates about reproductive freedoms are framed as fights over individual rights, it can engender a legal quagmire. Other entities with rights emerge – the fetus, for example, or a potential grandparent – and are pitted against the pregnant person.
Recently, for instance, a pregnant woman declared brain dead in Georgia was kept alive for several months until her fetus became viable, apparently to comply with the state’s strict anti-abortion law. As her mother told the press, her family had no say in the matter.
Narrowly focusing on abortion as an individual right can also obscure why banning it has societal impacts.
Research worldwide shows that restricting reproductive freedoms does not lead to fewer abortions. Abortion bans only make abortion dangerous as people turn to unregulated “back alley” procedures. Maternal and infant mortality rates rise, especially in marginalized communities.
Other kinds of suffering increase, too. Women and their families tend to become poorer when contraception and abortion are hard to get.
Abortion bans also lead to discriminatory practices in health care beyond reproductive health services, such as oncology, neurology and cardiology. Physicians who fear criminalization are forced to withhold or alter gold-standard treatments for pregnant patients, for example, or they may prescribe less effective drugs out of concern about legal consequences should patients later become pregnant.
As a result, abortion bans decrease the quality and effectiveness of medical care for many patients, not just those who are pregnant.
Defending reproductive freedoms for healthy democracies
These findings demonstrate why reproductive rights are really a collective good. When viewed this way, it illuminates why they are an essential element of democracy.
Already, the rollback of reproductive freedoms in the U.S. has been followed by efforts to limit other key areas of freedoms, including LGBTQ rights, freedom of speech and the right to travel.
Access to safe abortion for pregnant people, gender-affirming care for trans youth, and international travel for noncitizens are intertwined rights – not isolated issues.
When the government starts stripping away any of these rights, I believe it signals serious trouble for democracy.
This story is published in collaboration with Rewire News Group, a nonprofit newsroom dedicated to covering reproductive and sexual health.
At a Senate hearing on Sept. 9, 2025, on the corruption of science, witnesses presented an unpublished study that made a big assertion.
They claimed that the study, soon to be featured in a highly publicized film called “An Inconvenient Study,” expected out in early October 2025, provides landmark evidence that vaccines raise the risk of chronic diseases in childhood.
The study was conducted in 2020 by researchers at Henry Ford Health, a health care network in Detroit and southeast Michigan. Before the Sept. 9 hearing the study was not publicly available, but it became part of the public record after the hearing and is now posted on the Senate committee website.
At the hearing, Aaron Siri, a lawyer who specializes in vaccine lawsuits and acts as a legal adviser to Secretary of Health and Human Services Robert F. Kennedy Jr., said the study was never published because the authors feared being fired for finding evidence supporting the health risks of vaccines. His rhetoric made the study sound definitive.
As the head of biostatistics at the University of Pennsylvania’s Perelman School of Medicine, when I encounter new scientific claims, I always start with the question “Could this be true?” Then, I evaluate the evidence.
I can say definitively that the study by Henry Ford Health researchers has serious design problems that keep it from revealing much about whether vaccines affect children’s long-term health. In fact, a spokesperson at Henry Ford Health told journalists seeking comment on the study that it “was not published because it did not meet the rigorous scientific standards we demand as a premier medical research institution.”
The study’s weaknesses illustrate several key principles of biostatistics.
Study participants and conclusions
The researchers examined the medical records of about 18,500 children born between 2000 and 2016 within the Henry Ford Health network. According to the records, roughly 16,500 children had received at least one vaccine and about 2,000 were completely unvaccinated.
The authors compared the two groups on a wide set of outcomes. These included conditions that affect the immune system, such as asthma, allergies and autoimmune disorders. They also included neurodevelopmental outcomes such as attention-deficit/hyperactivity disorder, or ADHD, autism and speech and seizure disorders, as well as learning, intellectual, behavioral and motor disabilities.
Their headline result was that vaccinated children had 2.5 times the rate of “any selected chronic disease,” with 3 to 6 times higher rates for some specific conditions. They did not find that vaccinated children had higher rates of autism.
The study’s summary states it found that “vaccine exposure in children was associated with increased risk of developing a chronic health disorder.” That wording is strong, but it is not well supported given the weaknesses of the paper.
Timeline logic
To study long-term diseases in children, it’s crucial to track their health until the ages when these problems usually show up. Many conditions in the study, like asthma, ADHD, learning problems and behavior issues, are mostly diagnosed after age 5, once kids are in school. If kids are not followed that long, many cases will be missed.
However, that’s what happened here, especially for children in the unvaccinated group.
About 25% of unvaccinated children in the study were tracked until they were less than 6 months old, 50% until they were less than 15 months old, and only 25% were tracked past age 3. That’s too short to catch most of these conditions. Vaccinated kids, however, were followed much longer, with 75% followed past 15 months of age, 50% past 2.7 years of age and 25% past 5.7 years of age.
The longer timeline gave the vaccinated kids many more chances to have diagnoses recorded in their Henry Ford medical records compared with the nonvaccinated group. The study includes no explanation for this difference.
When one group is watched longer and into the ages when problems are usually found, they will almost always look sicker on paper, even if the real risks are the same. In statistics, this is called surveillance bias.
The primary methods used in the paper were not sufficient to adjust for this surveillance bias. The authors tried new analyses using only kids followed beyond age 1, 3 or 5. But vaccinated kids were still tracked longer, with more reaching the ages when diagnoses are made, so those efforts did not fix this bias.
More opportunities to be diagnosed
Not all cases of chronic disease are written down in the Henry Ford records. Kids who go to a Henry Ford doctor more often get more checkups, more tests and more chances for their diseases to be found and recorded in the Henry Ford system. Increased doctor visits has been shown to increase the chance of diagnosing chronic conditions, including autism, ADHD, asthma, developmental disorders and learning disabilities.
If people in one group see doctors more often than people in another, those people may look like they have higher disease rates even if their true health is the same across both groups. In statistics, this is called detection bias.
In the Henry Ford system, vaccinated kids averaged about seven visits per year, while unvaccinated kids had only about two. That gave the vaccinated kids many more chances to be diagnosed. The authors tried leaving out kids with zero visits, but this did not fix the detection bias, since vaccinated kids still had far more visits.
Another issue is that the study doesn’t show which kids actually used Henry Ford for their main care. Many babies are seen at the hospital for birth and early visits, but then go elsewhere for routine care. If that happens, later diagnoses would not appear in the Henry Ford records. The short follow-up for many children suggests a lot may have left the system after infancy, hiding diagnoses made outside Henry Ford.
Apples and oranges
Big differences between the groups of vaccinated and unvaccinated children can make it hard to know if vaccines really caused any differences in chronic disease. This is because of a statistical concept called confounding.
The two groups were not alike from birth. They differed in characteristics like sex, race, birth weight, being born early and the mother experiencing birth complications – all factors linked to later effects on health. The study made some adjustments for these, but left out many other important risks, such as:
• Whether families live in urban, suburban or rural areas.
• Family income, health insurance and resources.
• Environmental exposures such as air and water pollution, which were concerns in Detroit at that time.
Many factors can affect how often a child visits a health care provider.
These factors can affect both the chance of getting vaccinated and the chance of having health problems. They also change how often families visit Henry Ford clinics, which affects what shows up in the records.
When too many measured and unmeasured differences line up, as they do here, the study is unable to fully separate cause from effect.
Bottom line
The Henry Ford data could be helpful if the study followed both groups of kids to the same ages and took into account differences in health care use and background risks.
But as written, the study’s main comparisons are tilted. The follow-up time was short and uneven, kids had unequal chances for diagnosis, and the two groups were very different in ways that matter. The methods used did not adequately fix these problems. Because of this, the differences reported in the study do not show that vaccines cause chronic disease.
Good science asks tough questions and uses methods strong enough to answer them. This study falls short, and it is being presented as stronger evidence than its design really allows.
The Make America Healthy Again movement has generated a lot of discussion about public health. But the language MAHA proponents use to describe health and disease has also raised concerns among the disability and chronic illness communities.
I’m a researcher studying the rhetoric of health and medicine – and, specifically, the rhetoric of risk. This means I analyze the language used by public officials, institutions, health care providers and other groups in discussing health risks to decode the underlying beliefs and assumptions that can affect both policy and public sentiment about health issues.
As a scholar of rhetoric and the mother of an autistic child, in the language of MAHA I hear a disregard for the humanity of people with disabilities and a shift from supporting them to blaming them for their needs.
Such language goes all the way up to the MAHA movement’s highest-level leader, Health and Human Services Secretary Robert F. Kennedy Jr. It is clearly evident in the report on children’s health published in May 2025 by the MAHA Commission, which was established by President Donald Trump and is led by Kennedy, as well as in the MAHA Commission’s follow-up draft recommendations, leaked on Aug. 15, 2025.
One key concept for understanding the MAHA movement’s rhetoric, introduced by a prominent sociologist named Ulrich Beck, is what sociologists now call individualization of risk. Beck argued that modern societies and governments frame almost all health risks as being about personal choice and responsibility. That approach obscures how policies made by large institutions – such as governments, for example – constrain the choices that people are able to make.
In other words, governments and other institutions tend to focus on the choices that individuals make to intentionally deflect from their own responsibility for the other risk factors. The consequence, in many cases, is that the institution is off the hook for any responsibility for negative outcomes.
Beck, writing in 1986, pointed to nuclear plants in the Soviet Union as an example. People who lived near them reported health issues that they suspected were caused by radiation. But the government denied the existence of any evidence linking their woes to radiation exposure, implying that lifestyle choices were to blame. Some scholars have identified a similar dynamic in the U.S. today, where the government emphasizes personal responsibility while downplaying the effects of public policy on health outcomes.
A shift in responsibility
Such a shift in responsibility is evident in how MAHA proponents, including Kennedy, discuss chronic illness and disabilities – in particular, autism.
In its May 2025 report on children’s health, the MAHA Commission describes the administration’s views on chronic diseases in children. The report notes that the increased prevalence in “obesity, diabetes, neurodevelopmental disorders, cancer, mental health, autoimmune disorders and allergies” are “preventable trends.” It also frames the “major drivers” of these trends as “the food children are eating, the chemicals they are exposed to, the medications they are taking, and various changes to their lifestyle and behavior, particularly those related to physical activity, sleep and the use of technology.”
Extensive research shows that genetics accounts for most of the risk of developing autism, but the MAHA Commission report discussed only lifestyle and environmental factors. Dusan Stankovic/E+ via Getty Images
There’s nothing inherently wrong with studying the environmental factors that might contribute to autism or other neurodevelopmental disorders. In fact, many researchers believe that autism is caused by complex interactions between genes and environmental factors. But here’s where Beck’s concept of individualization becomes revealing: While the government is clearly not responsible for the genetic causes of chronic diseases, this narrow focus on lifestyle and environmental factors implies that autism can be prevented if these factors are altered or eliminated.
While this may sound like great news, there are a couple of problems. First, it’s simply not true. Second, the Trump administration and Kennedy have canceled tens of millions of dollars in research funding for autism – including on environmental causes – replacing it with an initiative with an unclear review process. This is an unusual move if the goal is to identify and mitigate environmental risk factors And finally, the government could use this claim to justify removing federally funded support systems that are essential for the well-being of autistic people and their families – and instead focus all its efforts on eliminating processed foods, toxins and vaccines.
Even more worrisome is the implication that autism is a kind of damage caused by the environment rather than one of many normal variations in human neurological diversity – framing people with autism as a problem that society must solve.
How language encodes value judgments
Such logic sets off alarm bells for anyone familiar with the history of eugenics, a movement that began with the idea of improving America by making its people healthier and quickly evolved to make judgments about who is and is not fit to participate in society.
Kennedy’s explanation for the rise in autism diagnoses contradicts decades of research by independent researchers as well as assessments by the CDC.
Even if organic foods and a toxin-free household were the answer to reducing the prevalence of autism, the leaked MAHA Commission strategy report steers clear of recommending government regulation in industries such as food and agriculture, which would be needed to make these options affordable and widely available.
Instead, MAHA’s supposed interventions would remain lifestyle choices – and expensive ones, at that – left for individual families to make for themselves.
Just asking questions
Kennedy and other MAHA proponents also employ another powerful rhetorical tactic: raising questions about topics that have already reached a scientific consensus. This tactic frames such questions as pursuits of truth, but their purpose is actually to create doubt. This tactic, too, is evident in the MAHA Commission’s reports.
MAHA rhetoric thus continues a troubling trend in the anti-vaccine movement of calling all of science and Western medicine into question in order to further a specific agenda, regardless of the risks to public health.
The MAHA Commission’s goals are almost universally appealing – healthier food, healthier kids and a healthier environment for all Americans. But analyzing what is implied, minimized or left out entirely can illuminate a much more complex political and social agenda.
Now, a new study that we conducted with a team of colleagues suggests that dogs might have a deeper and more biologically complex effect on humans than scientists previously believed. And this complexity may have profound implications for human health.
How stress works
The human response to stress is a finely tuned and coordinated set of various physiological pathways. Previous studies of the effects of dogs on human stress focused on just one pathway at a time. For our study, we zoomed out a bit and measured multiple biological indicators of the body’s state, or biomarkers, from both of the body’s major stress pathways. This allowed us to get a more complete picture of how a dog’s presence affects stress in the human body.
When a person experiences a stressful event, the SAM axis acts quickly, triggering a “fight or flight” response that includes a surge of adrenaline, leading to a burst of energy that helps us meet threats. This response can be measured through an enzyme called alpha-amylase.
At the same time, but a little more slowly, the HPA axis activates the adrenal glands to produce the hormone cortisol. This can help a person meet threats that might last for hours or even days. If everything goes well, when the danger ends, both axes settle down, and the body goes back to its calm state.
While stress can be an uncomfortable feeling, it has been important to human survival. Our hunter-gatherer ancestors had to respond effectively to acute stress events like an animal attack. In such instances, over-responding could be as ineffective as under-responding. Staying in an optimal stress response zone maximized humans’ chances of survival.
After cortisol is released by the adrenal glands, it eventually makes its way into your saliva, making it an easily accessible biomarker to track responses. Because of this, most research on dogs and stress has focused on salivary cortisol alone.
While these studies have shown that having a dog nearby can lower cortisol levels during a stressful event, suggesting the person is calmer, we suspected that was just part of the story.
What our study measured
For our study, we recruited about 40 dog owners to participate in a 15-minute gold standard laboratory stress test. This involves public speaking and oral math in front of a panel of expressionless people posing as behavioral specialists.
The participants were randomly assigned to bring their dogs to the lab with them or to leave their dogs at home. We measured cortisol in blood samples taken before, immediately after and about 45 minutes following the test as a biomarker of HPA axis activity. And unlike previous studies, we also measured the enzyme alpha-amylase in the same blood samples as a biomarker of the SAM axis.
As expected based on previous studies, the people who had their dog with them showed lower cortisol spikes. But we also found that people with their dog experienced a clear spike of alpha-amylase, while those without their dog showed almost no response.
No response may sound like a good thing, but in fact, a flat alpha-amylase response can be a sign of a dysregulated response to stress, often seen in people experiencing high stress responses, chronic stress or even PTSD. This lack of response is caused by chronic or overwhelming stress that can change how our nervous system responds to stressors.
In contrast, the participants with their dogs had a more balanced response: Their cortisol didn’t spike too high, but their alpha-amylase still activated. This shows that they were alert and engaged throughout the test, then able to return to normal within 45 minutes. That’s the sweet spot for handling stress effectively. Our research suggests that our canine companions keep us in a healthy zone of stress response.
Having a dog benefits humans’ physical and psychological health.
Dogs and human health
This more nuanced understanding of the biological effects of dogs on the human stress response opens up exciting possibilities. Based on the results of our study, our team has begun a new study using thousands of biomarkers to delve deeper into the biology of how psychiatric service dogs reduce PTSD in military veterans.
But one thing is already clear: Dogs aren’t just good company. They might just be one of the most accessible and effective tools for staying healthy in a stressful world.
In today’s digital world, people routinely turn to the internet for health or medical information. In addition to actively searching online, they often come across health-related information on social media or receive it through emails or messages from family or friends.
It can be tempting to share such messages with loved ones – often with the best of intentions.
Although there is a fire hose of health-related content online, not all of it is factual. In fact, much of it is inaccurate or misleading, raising a serious health communication problem: Fake health information – whether shared unknowingly and innocently, or deliberately to mislead or cause harm – can be far more captivating than accurate information.
This makes it difficult for people to know which sources to trust and which content is worthy of sharing.
The allure of fake health information
Fake health information can take many forms. For example, it may be misleading content that distorts facts to frame an issue or individual in a certain context. Or it may be based on false connections, where headlines, visuals or captions don’t align with the content. Despite this variation, such content often shares a few common characteristics that make it seem believable and more shareable than facts.
Another marker of fake health information is that it presents ideas that are simply too good to be true. There is something appealingly counterintuitive in certain types of fake health information that can make people feel they have access to valuable or exclusive knowledge that others may not know. For example, a claim such as “chocolate helps you lose weight” can be especially appealing because it offers a sense of permission to indulge and taps into a simple, feel-good solution to a complex problem. Such information often spreads faster because it sounds both surprising and hopeful, validating what some people want to believe.
In a study on vaccine hesitancy published in 2020, my colleagues and I found that controversial headlines in news reports that go viral before national vaccination campaigns can discourage parents from getting their children vaccinated. These headlines seem to reveal sensational and secret information that can falsely boost the message’s credibility.
The pull to share
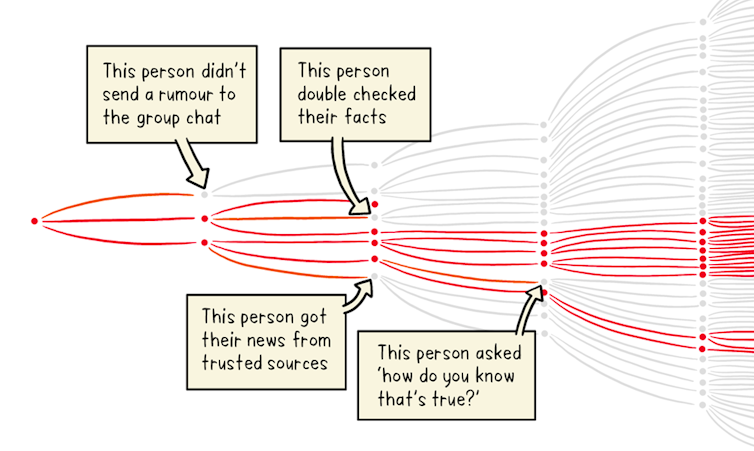
The internet has created fertile ground for spreading fake health information. Professional-looking websites and social media posts with misleading headlines can lure people into clicking or quickly sharing, which drives more and more readers to the falsehood. People tend to share information they believe is relevant to them or their social circles.
In 2019, an article with the false headline “Ginger is 10,000x more effective at killing cancer than chemo” was shared more than 800,000 times on Facebook. The article contained several factors that make people feel an urgency to react and share without checking the facts: compelling visuals, emotional stories, misleading graphs, quotes from experts with omitted context and outdated content that is recirculated.
Visual cues like the logos of reputable organizations or photos of people wearing white medical coats add credibility to these posts. This kind of content is highly shareable, often reaching far more people than scientifically accurate studies that may lack eye-catching headlines or visuals, easy-to-understand words or dramatic storylines.
How to combat the spread of fake health information
In today’s era of information overload in which anyone can create and share content, being able to distinguish between credible and misleading health information before sharing is more important than ever. Researchers and public health organizations have outlined several strategies to help people make better-informed decisions.
Whether health care consumers come across health information on social media, in an email or through a messaging app, here are three reliable ways to verify its accuracy and credibility before sharing:
Evaluate the source’s credibility. A quick way to assess a website’s trustworthiness is to check its “About Us” page. This section usually explains who is behind the content, their mission and their credentials. Also, search the name of the author. Do they have recognized expertise or affiliations with credible institutions? Reliable websites often have domains ending in .gov or .edu, indicating government or educational institutions. Finally, check the publication date. Information on the internet keeps circulating for years and may not be the most accurate or relevant in the present context.
If you’re still unsure, don’t share. If you’re still uncertain about the accuracy of a claim, it’s better to keep it to yourself. Forwarding unverified information can unintentionally contribute to the spread of misinformation and potentially cause harm, especially when it comes to health.
Questioning dubious claims and sharing only verified information not only protects against unsafe behaviors and panic, but it also helps curb the spread of fake health information. At a time when misinformation can spread faster than a virus, taking a moment to pause and fact-check can make a big difference.
I used to answer questions on Livejournal. Most of the time, people wanted to know about matters historical, especially concerning the Middle Ages. When I moved to a blog on my own website, that interaction lessened somewhat and I stopped asking if anyone had questions they wanted me to answer.
I discovered this summer (for yes, it’s still summer in Australia) that I missed that interaction with readers. I asked on Facebook if anyone had any questions they’d like me to answer here. The people of Facebook answered. There were several simple questions (or questions with simple answers) and I’ll reply to them today, but there were two questions that demand more complex answers, so they’ll be posts of their own.
Before I answer those two questions, I would be delighted if anyone reading this have questions of your own. Ask them in the comments.
I’m happy to take questions about Australia and our history, my family history, Australian Jews, Judaism in general, the Middle Ages in Western Europe, medieval magic, food history, my favourite anime, Doctor Who, my writing, my current projects, dealing with many illnesses at once, any of the subjects linked to any of my doctorates, and… to be honest… anything else I have an interest in except certain current issues.
I don’t answer questions about Israel partly because there are others who know a lot more but mostly because I don’t like bullies and there are a lot of people demanding right now “Deny any links to Israel in your family and your Jewish heritage and religion and then we might speak to you.” This is bullying. Also, the fact that I spell out the demand in this particular way says a bunch about my views, so now you don’t need to ask those questions!
Also, I am not going to answer questions at this time (maybe other places and times) about family physically hurt and even killed due to antisemitism and related hate. I don’t have the spoons. I do have such family and the pain I feel for them never stops. And no, this does not mean I don’t care about anyone outside my family. I’m capable of caring for family and for a whole bunch of other people also, oddly. I don’t want to answer questions about them because most of the people who ask such questions have particular platforms and… I do not want the questions to play with emotions and safety. Besides, aren’t my regular subjects sufficiently interesting?
Today I’ll be answering two questions, and they’re quite different from each other. Even if the readers are also friends, I won’t use their names. Privacy matters. If you want to identify yourself, feel free to in the comments.
A reader said, “Oh, I do have a question! It just occurred to me when I was looking at pictures of beautiful menorahs on Bluesky last week. If someone can’t physically light their menorah because of illness or disability, can they use one with battery operated candles. And more generally, how do the rules around not working or using modern technology on the Sabbath work for disabled Jews who want to observe that but need technology to be independent, and don’t have outside support?”
The answer is both simple and complex. Judaism is not a one-size-fits-all religion. We’re taught a bunch of questions we can ask ourselves and make our own decisions about such things, and we can also ask rabbis. Health and well-being matter to us, so if we need a mechanical help then we are not encouraged to forgo it during Shabbat. The decision comes down to the person whose body it is, or, in the case of lighting candles for Chanukah, whose chanukiya it is.
I was taught from my childhood that we’re responsible for our own decisions and that it’s always better if those decisions are informed. For any Jew brought up as I was, there are choices on how to become informed. Some people rely heavily on the views of rabbis. Some read up a lot. Some simply make up their mind what to do and when.
Most of the time, for something like lighting candles, pragmatism rules, I suspect. I can’t speak on behalf of others and tell you what choices they make. Because our understanding of the world and of Judaism matters, decisions on these matters can be hugely varied. Some Jews are so enormously religious that every choice in life requires immense thought and respect paid to both the letter of the law and the spirit of the law. Some are casual about the religious side and may not light the candles at all, because they have other things to do with limited capacity. Most of us are somewhere in between.
Even for those of us who fall into the in-between land, the can be huge differences. One of the wonderful things about Judaism is these differences. When I talk to other Jews I find out their traditions and we chat about the reasons behind this choice or that. Learning is part of the Jewish soul and so learning about choices, whether they be choices for how to remain a good human being or choices about the lighting of candlesticks will always throw up interesting insights.
Let me leave you with one of my favourite candle-lighting insights from my childhood. There is a perpetual light inside synagogues. This light reminds us of the holy light that was always kept lit in the Temple. That original light is the reason for the miracle needed on the original days of Chanukah, when that light had to be kept going even when there was no clean oil to keep it going with because so much had been defiled by the worship of a different religion entirely within our holiest of holies. Lo, the oil lasted eights days. Celebrating that light from the Temple before its destruction led eventually to the candles we light for Chanukah. The original light was in an oil lamp, and for a very long time oil and wicks gave us our Chanukah lights. Now, most of us use candles for Chanukah (as you know) and electricity for the memory of the Ner Tamid.
The other question I’ll answer this week is quite, quite different. “So, I know you have some extremely talented, but – it’s fair to say – vastly different, musicians in your family history. What is your favourite musical memory from one of your family members?”
Normally I’d give a story about my father’s first cousin, Linda Phillips. Not only was she the per-eminent musician in the family, but she had great stories. Or I’d tell you about my own first cousin, Jon Snyder, who played in Captain Matchbox. My most favourite of all the music stories in my family is all about my father.
My father was a dentist. He claimed he loved going to orchestral concerts because the music gave him a good nap. He was also tone deaf. The first and third sentences are the critical ones in this story.
My sisters and I helped out at the dental practice when we were old enough. We were called “Assistant Dental Nurses.” I was the one responsible for patients who found going to the dentist difficult. I was that person long before I was old enough to be an Assistant Dental Nurse. I was expected to go into the waiting room and chat with people. I was, when I did this, the first stage of my father’s very distinctive version of an anesthetic system. Also, when a patient hurt too much and panicked in the dental chair, I was sent to the waiting room to explain what was happening. A few lucky indivuals react, for instance, to nitrous oxide by making noises that sound as if aliens were burrowing into their skull. Dad always took these patients out from under the nitrous oxide and checked to see if they were fine.
With one patient in particular, she was perfectly fine, both times he checked. She had been telling Dad how fine she was, the first time, and the second, she was singing. She simply had no vocal chord control and she wasn’t listening to what she sounded like and… everyone in the waiting room was freaked out.
I was a teenager and very literal. I still am very literal. My explanation of what was happening, including the warning that this filling might take a little longer than we expected, didn’t just calm people down, they chuckled.
When each of those patients reached the dental chair, they were perfectly relaxed. Then Dad gave his list of choices for anesthesia.
1. No anesthetic at all. Quite a few people opted for this. I did, myself, when I could. These days I am weak as a kitten and need help.
2. Nitrous oxide, or laughing gas. It relaxes me, and no undue and unexpected screaming has ever resulted from me taking it. It’s what I accepted on bad days or if the filling was deep and my teeth sensitive.
3. An injection.
4. A series of jokes by Dad. No-one ever chose this option, because everyone knew my father’s sense of humour. His favourite photocopy jokes were all on display in the waiting room.
5. A rap over the head with a hammer. No-one ever chose this, either.
6. Dad singing them to sleep. Some people chose this. When they realised that Dad sang in many keys, but only used two notes, they stopped him and said “How about we try an injection?”
To be honest, Dad’s list changed according to his mood. Once it reached 9 items, but I can’t remember them.
I do remember the time he decided to sing “Maxwell’s Silver Hammer” and the patient asked him if he had an invisible hand, holding the hammer, because he hurt so much from the singing that death might be preferable. From then, when I was Assistant Dental Nurse, I warned people in the waiting room about the list and said, “No matter what you do, don’t let Dad sing.”
People are asking me “Are you going to Belfast next year?” and “Are you going to Seattle?” and “Will you return to Germany?” and “Do we get to see you in person in Baltimore?” I always explain to European friends and North American friends that the airfares are large and more and more often they reply, “Well, it’s difficult for me, too.” And it is.
Yet the obstacles appear, to me, higher than they were.
I wondered if I was shouting about fire when it was merely a match that was burning. I know that my recent trip was difficult because I needed more physical help than I could afford. Several friends stepped up and made it happen, but there were too many times when I was nearly stranded with no recourse, simply because of the health issues. I still have nightmares about 5 moments that were well-nigh impossible.
For any future trip that takes more than 8 hours, I will need help at the other end and along the way. I have to accept that I cannot do things alone easily, even things that look perfectly straightforward to other people.
Shouting at me, “Get a scooter” when I’m struggling at a science fiction conference does not help, and (what happened a lot in Germany) someone walking by stopping to pick up my bag and get it over the hump or up the steps helps immensely. Neither of these are standard for any trip, but they’re what I experienced. Five times in one day in Glasgow I was told to get a scooter or a wheelchair, when, in fact, if I’d done that I’d have been unable to walk at all long term (or even a few days after).
This is not the first time that strangers and friends alike wanted to treat me in the way they thought chronically ill and disabled people should be treated and not consider (or even ask about) my actual circumstances. Because I can walk a little, most friends would say, “Come with me” and leave me at the other end with no thought that, since I had not planned to get to that place, I had no way of getting back in time for programme or for transport: I have to plan.
All this means is that I have to plan more when I travel. I need to be able to see what I can do and then achieve it.
I had to cancel visits to key sites in Germany because the world and my health simply did not permit it.
I had to cancel a half day at Glasgow because there were problems with a room for the panel I was on. All I needed to do to make everything work, was to sit. Not to sit and move and sit and move and sit and move – just to sit. Standing had fewer after-effects, so I stood and awaiting until the re-assigned room could be replaced with something else and the missing computer could also be replaced. All this happened, and was a miracle of reorganisation, but I had not sat when I had planned to. I could have done it on a panel or in a lounge chair, but intermittent movement with that particular pain meant that after that panel, I missed everything that didn’t take place in a single comfortable chair. I was not even able to walk back to the hotel and lie down. I was very lucky that afternoon because a friend stayed with me and we had a lovely evening and she got drinks and found mutual friends and… listened and paid attention to what I was saying about what I could do. She also made sure I got safely back to the hotel at the end of the evening, which was not a given because my direction sense fails when I am at that point of pain. Also, she did not treat me as a charity case, but as a delightful friend and who she was happy to spend time with. This friend resulted in there being no sour taste in my mouth from my incapacity. She’s wonderful. I did miss 8 hours of programming I had intended to enjoy, however.
All these are reasons for being careful how I travel, not avoiding long-distance travel entirely.However, I’ve now acquitted all the grants I was given to get to Europe. I took a moment to do some calculations after the last form went through.
In future, I don’t think I can get further than New Zealand without financial help. The recent trip cost the equivalent of 45% of my annual income. That was without adding enough assistance to make the trip at all comfortable, (which is what I was unable to do this time) and I’m still paying physically for the return journey. I could only pay that amount with help from the friends I stayed with and from the bodies that gave me grants, and, if I wanted an equivalent trip to anywhere in Europe or North America for a conference or for research without as many problems, it would cost me 60% of my annual income.
Without grants it’s just not possible. That’s easy to explain. What is not easy to explain is that many non-academic programmes and some academic programmes are pulled together at the last minute in these days of everyone working with too much pressure. If I’m not giving an academic paper or on programme, I cannot claim that amount on taxes. If I do not know about programme early enough, that adds $1,000-3,000 to the total cost of the trip because airlines play games with last minute travellers who need to arrange things carefully so that they don’t hurt for weeks. That brings the cost potentially to over 55% of my income if I go the route that hurts, and over 70% if I plan to hurt much less.
I will miss everyone, but I can’t travel long distances under these circumstances, however much I adore being with people and researching and discovering amazing things and listening to brilliant people. Also, the next person from Europe or North America who claims the same experience will be sympathised with, because over 45-70% of one’s income for one journey is quite scary.
If anyone has solutions and would like to see me in person, I would love to talk. In the interim, please just say “I’m sorry – I wish you could do these things” rather than telling me “I suffer just as much as you” while planning your next trip.